The reality inside most clinical settings involves 12-hour shifts, emotionally devastating patient outcomes, moral dilemmas with no clean answers, and a professional culture that treats asking for help as weakness. Chronic stress isn't an occasional challenge in healthcare—it's baked into the work itself.
The numbers reflect this. According to a 2023 study published in Mayo Clinic Proceedings, 45.2% of US physicians reported at least one burnout symptom—and among nurses, the American Nurses Foundation found that figure climbs to 56%. This isn't a wellness problem. It's a workforce crisis.
And it doesn't stay contained to the people experiencing it. Burned-out clinicians make more errors, disengage from patients, and leave the field—creating strain on the colleagues left behind.
This guide covers what burnout actually is (and how it differs from stress), why healthcare workers face uniquely high risk, proven individual strategies, the case for mental fitness as a proactive approach, and what organizations must change to make prevention possible.
TL;DR
- Burnout is a WHO-classified, three-part syndrome (exhaustion, depersonalization, reduced efficacy) that rest alone won't fix.
- Structural stressors like moral injury, documentation overload, and understaffing go beyond what individual coping can handle.
- Mindfulness-based stress reduction, CBT-based skills, sleep protection, and peer support all show measurable results in clinical populations.
- Lasting prevention requires both individual practice and organizational change—neither works without the other.
Burnout vs. Stress: What Healthcare Professionals Need to Know
The Clinical Distinction
Occupational stress is a normal physiological response to workplace demands. It can actually sharpen performance in short bursts. Burnout is something different altogether.
The WHO classifies burnout under ICD-11 as an occupational phenomenon—not a medical diagnosis—resulting from chronic workplace stress that hasn't been successfully managed. It has three distinct dimensions, as defined by the Maslach Burnout Inventory (MBI), the field's standard measurement tool:
- Emotional exhaustion — persistent depletion that sleep doesn't restore
- Depersonalization — cynicism, detachment, or emotional numbness toward patients and work
- Reduced personal accomplishment — feeling ineffective despite sustained effort
The key distinction: stress tends to resolve when the stressor passes. Burnout doesn't.
How Burnout Develops
The progression follows a recognizable slope. Early enthusiasm gives way to stagnation, then frustration, then apathy — and eventually full burnout. Most people don't notice it happening because each stage feels like a reasonable response to difficult circumstances.
In healthcare, this pattern is especially dangerous because the early warning signs are routinely normalized:
- Fatigue that doesn't lift after days off
- Irritability or emotional blunting toward patients
- Feeling like your work doesn't matter regardless of outcome
- Physical symptoms—headaches, GI issues, chronic sleep disruption
- Reduced empathy that once came naturally
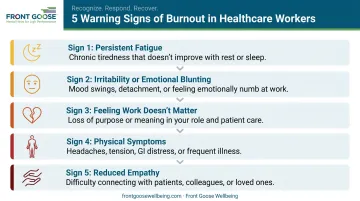
When a culture treats these symptoms as signs of dedication rather than distress, they go unaddressed until the damage is severe.
Moral Injury: A Healthcare-Specific Accelerant
Not all healthcare exhaustion is burnout. Moral injury is a distinct but related condition — it occurs when healthcare workers are prevented from acting in accordance with their ethical values. Common triggers include:
- Rationing care due to resource constraints
- Spending more time on documentation than with patients
- Watching a system fail people you're trying to help
Recognizing moral injury matters because it requires different interventions. You can't breathe your way out of a systemic problem. Identifying whether exhaustion stems from workload, values violation, or both shapes what kind of support actually helps.
Why Healthcare Workers Face Uniquely High Burnout Risk
Structural Stressors That Compound Over Time
Most professions have stressful days. Healthcare has a structural architecture that makes chronic stress nearly unavoidable:
- High patient volumes with inadequate staffing
- Life-and-death decision-making under time pressure
- Repeated exposure to suffering, trauma, and death
- Long, irregular hours with limited recovery time
- Administrative burden: ambulatory physicians spend nearly 50% of their time on EHR and desk work versus just 27% in direct patient care
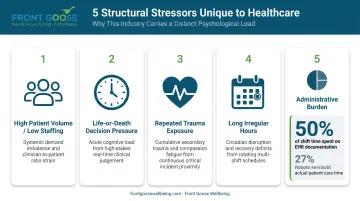
When nearly half a physician's workday goes to documentation rather than the work they trained for, the gap between purpose and reality widens daily.
The Help-Seeking Problem
Healthcare culture makes burnout worse by making it harder to acknowledge. The expectation of self-sufficiency runs deep. Admitting struggle can feel like professional failure, and in many cases it carries concrete professional risk.
A Mayo Clinic Proceedings study of 5,829 physicians found that 40% were reluctant to seek mental health care due to concerns about licensure repercussions. This isn't irrational fear. Credentialing and licensing questions about mental health history exist in many states, creating a structural disincentive to get help. COVID-19 sharpened all of this: physician burnout spiked to 62.8% in 2021, up from 38.2% the previous year. The culture of sacrifice praised during the pandemic didn't dissolve when the acute crisis passed.
The Patient Safety Connection
Burnout isn't only a staff wellbeing issue. A BMJ meta-analysis of 170 studies involving 239,246 physicians found burnout associated with twice the odds of patient-safety incidents (OR 2.04). Burned-out clinicians have higher error rates, lower professional engagement, and worse patient satisfaction scores.
This cycle compounds quickly: burned-out teams make more errors, which adds stress, which accelerates burnout on already short-staffed units. Preventing burnout is, at its foundation, a patient safety strategy.
Science-Backed Strategies to Manage Stress and Prevent Burnout
Mindfulness and MBSR
Mindfulness-Based Stress Reduction has the strongest direct evidence for healthcare workers. A JAMA Network Open RCT found that a brief mindfulness program significantly reduced perceived stress compared to controls (17.29 vs. 18.54, p=.02). Systematic reviews of MBSR in healthcare populations consistently show reductions in anxiety, depression, and emotional exhaustion.
What makes MBSR practical for shift workers: even 10–15 minutes of daily practice produces measurable results. The practice doesn't require silence or a yoga mat—body scans and breathing exercises work during a commute, before a shift, or in a break room.
CBT-Based Skills and Psychological Flexibility
Cognitive-behavioral approaches help clinicians identify and interrupt unhelpful thought cycles. In high-stakes environments, these patterns are common drivers of emotional exhaustion:
- Catastrophizing patient outcomes after difficult cases
- All-or-nothing thinking about clinical performance
- Rumination that persists long after a shift ends
Acceptance and Commitment Therapy (ACT) offers a complementary angle. Rather than eliminating difficult thoughts, it builds psychological flexibility: the ability to act in alignment with your values even when circumstances are hard. For healthcare workers facing moral injury, that distinction matters.
Boundaries and Micro-Recovery
Boundary-setting is a skill, not a personality trait. Specific, learnable behaviors include:
- Limiting after-hours availability to genuine emergencies
- Delegating non-clinical administrative tasks where possible
- Building protected transition time between demanding patient interactions
"Micro-recovery" deserves particular attention. These are brief, intentional breaks — 5 to 10 minutes of genuine disengagement during a shift — that interrupt cortisol accumulation before stress cascades into physical and cognitive fatigue. Rest breaks are most effective when management actively normalizes and protects them — not just permits them in policy.
Sleep and Physical Foundations
Sleep may be the single most undervalued burnout prevention tool in healthcare. Sleep-deprived ICU interns made approximately 36% more serious medical errors in early research. More recent reviews find sleep loss contributes to errors in 37–40% of both attending and trainee physicians.
The practical targets:
- 7–9 hours, with schedule consistency being as important as total quantity
- Regular physical activity (even brief daily movement) to regulate cortisol
- Nutrition that supports sustained cognitive function across long shifts

Peer Support and Social Connection
Isolation accelerates burnout. Having colleagues who understand the specific weight of clinical work is a genuine protective factor. Structured peer support programs — particularly those developed in the wake of COVID-19 — have demonstrated meaningful reductions in burnout and trauma symptoms among healthcare workers.
Informal connection carries real weight too. Regular check-ins, mentorship relationships, and normalized conversations about difficult cases all reduce the compounding effect of carrying clinical stress alone.
Mental Fitness Training: A Proactive Approach
Beyond Coping: Building Capacity
Mental fitness is distinct from mental health treatment. Treatment addresses dysfunction; mental fitness builds capacity before dysfunction develops. The analogy to physical training is direct: you don't wait until you can't walk to start exercising.
The neuroscience behind this is well-established. An 8-week MBSR program produced measurable increases in gray matter concentration in brain regions linked to learning, memory, and emotional regulation. Meditation practice has been associated with increased cortical thickness in prefrontal regions involved in decision-making, and with reduced amygdala reactivity to stress. These are structural changes in the organ that manages stress response — not metaphors.
Core Pillars of Mental Fitness for Healthcare Professionals
| Pillar | What It Builds |
|---|---|
| Resilience | Capacity to recover from setbacks without losing purpose |
| Emotional regulation | Recognizing and managing reactions before they drive behavior |
| Cognitive flexibility | Shifting perspective and problem-solving under pressure |
| Self-compassion | Extending to yourself the same care you extend to patients |

Each of these is trainable. None develops automatically under stress.
What Effective Mental Fitness Training Looks Like
One-off wellness workshops don't produce lasting change. Research on corporate training finds that 70% of training failure stems from lack of follow-up—and that without reinforcing activities, up to 90% of new skills disappear within a year. Healthcare burnout prevention programs that end after a single session reflect the same failure pattern.
Effective programs are built differently:
- Practice breathwork, body scans, and mindful awareness daily — consistency matters more than session length
- Identify and reframe thought patterns that amplify stress before they drive behavior
- Rehearse responses to high-pressure scenarios mentally before they occur in real time
- Reinforce learning through group coaching, structured reflection, and goal-setting over time
Front Goose Wellbeing's programs follow this structure. Founder Megan Dittman — a Certified Meditation Instructor (Chopra Institute), Board Certified Health & Wellness Coach (NBC-HWC), and Neuroleadership-certified coach — builds programs around three interconnected capacities: mindful awareness, mindset, and mental rehearsal. The reinforcement is built in, not bolted on.
For healthcare organizations, programs adapt to shift schedules, team structures, and the specific pressures clinical environments create.
What Healthcare Organizations Must Do: Systemic Solutions
The Limits of Individual Intervention
Individual tools help. But they can't outpace an organization that keeps generating the conditions for burnout.
The National Academy of Medicine is direct: clinician burnout requires a systems approach. When physicians spend half their day on documentation, when units are chronically understaffed, when reporting mental health concerns carries licensing risk—no amount of meditation closes that gap. Making resilience training the primary response to systemic problems shifts responsibility onto individuals who are already overloaded.
Evidence-Based Organizational Interventions
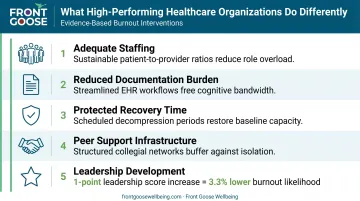
Organizations with lower burnout rates tend to share common structural features:
- Adequate staffing: removing the baseline pressure that makes every shift an emergency
- Reduced documentation burden: streamlining EHR workflows, adding scribes or support staff, auditing non-clinical administrative requirements
- Protected recovery time: designated breaks, manageable patient loads, reasonable shift scheduling
- Peer support infrastructure: formal programs that make psychological support available without stigma
- Leadership development: a Mayo Clinic Proceedings review found that every 1-point increase in leadership score was associated with 3.3% lower burnout likelihood and 9% higher satisfaction among physicians
Manager behavior isn't a soft cultural factor—it's a measurable driver of team burnout.
Building a Mental Health-Supportive Culture
Culture change requires more than policy. Specific practices that shift organizational culture around mental health:
- Leaders who model help-seeking openly and without penalty
- Zero tolerance for stigma around mental health conversations
- Employee Assistance Programs that are genuinely accessible and confidential
- Regular structured check-ins on team wellbeing—not just performance metrics
- Partnerships with external programs that deliver structured, science-backed training
Front Goose Wellbeing works with healthcare organizations to deliver exactly this kind of structured support: group-based mental fitness programs combining instructor-led breathwork, meditation, and stress management training with group coaching that builds shared accountability and lasting behavioral change.
The Business Case for Healthcare Leaders
Burnout prevention is a strategic and financial imperative. A JAMA Internal Medicine model estimated $4.6 billion in annual US costs attributable to physician burnout-related turnover and reduced clinical hours alone. That figure doesn't include nursing turnover—where 39% of surveyed nurses report intent to leave their position.
The return on investment from prevention is measurable:
- Lower recruitment and onboarding costs from reduced turnover
- Fewer medical errors and associated liability
- Improved patient outcomes and satisfaction scores
- Higher team performance and sustainable productivity
Organizations that act on this data start with a workplace needs assessment: identifying which stressors are structural, which are cultural, and which can be addressed through individual skill-building. From there, effective programs require genuine management buy-in, clear outcome measurement, and consistent delivery over time. A single training day won't shift a burnout culture. Sustained commitment will.
Frequently Asked Questions
What are the three main signs of burnout in healthcare workers?
The three core dimensions are emotional exhaustion (persistent depletion), depersonalization (cynicism or detachment toward patients and work), and reduced personal accomplishment (feeling ineffective despite effort). These are the criteria recognized by the WHO and measured by the Maslach Burnout Inventory.
How is occupational stress different from burnout?
Stress is a response to a specific demand and typically resolves when that demand passes. Burnout is a chronic syndrome that develops gradually from unmanaged stress and doesn't resolve with rest alone. Early recognition is what separates a manageable problem from a prolonged one.
Can healthcare worker burnout affect patient safety?
Yes, directly. A BMJ meta-analysis of over 239,000 physicians found burnout associated with twice the odds of patient-safety incidents. Burned-out clinicians show higher medical error rates, reduced professional engagement, and lower patient satisfaction — outcomes that affect care quality as much as staff health.
What is the most effective intervention for preventing burnout in healthcare?
Research consistently supports a combined approach: individual strategies (mindfulness, CBT-based coping, sleep protection, peer support) alongside organizational changes (workload management, leadership development, reduced administrative burden). Neither works reliably without the other.
How can a healthcare organization create a culture that prevents burnout?
Start with leadership modeling. Managers who openly prioritize wellbeing signal that it's safe for others to do the same. Pair that with adequate staffing, reduced documentation load, accessible mental health resources, and wellness programs built around ongoing reinforcement — not one-off events.
How long does it take to recover from healthcare burnout?
Recovery timelines vary depending on severity and whether the underlying conditions change, but meaningful improvement typically requires months of consistent intervention. Proactive mental fitness training — before full burnout sets in — is considerably faster and more effective than trying to recover after the fact.